Metatarsalgia vs Morton’s Neuroma: How to Tell the Difference
Metatarsalgia vs Morton’s Neuroma: How to Tell the Difference
Ball of foot pain can come from two very different conditions: metatarsalgia and Morton’s neuroma. They are often confused because both cause pain in the forefoot, but they involve different tissues and require different treatment approaches. This guide explains the difference, gives you a simple home test to identify which you have, and explains how to treat each condition effectively.
Key Takeaways
- Metatarsalgia is inflammation of the metatarsal bones; Morton’s neuroma is a benign nerve thickening between the toes
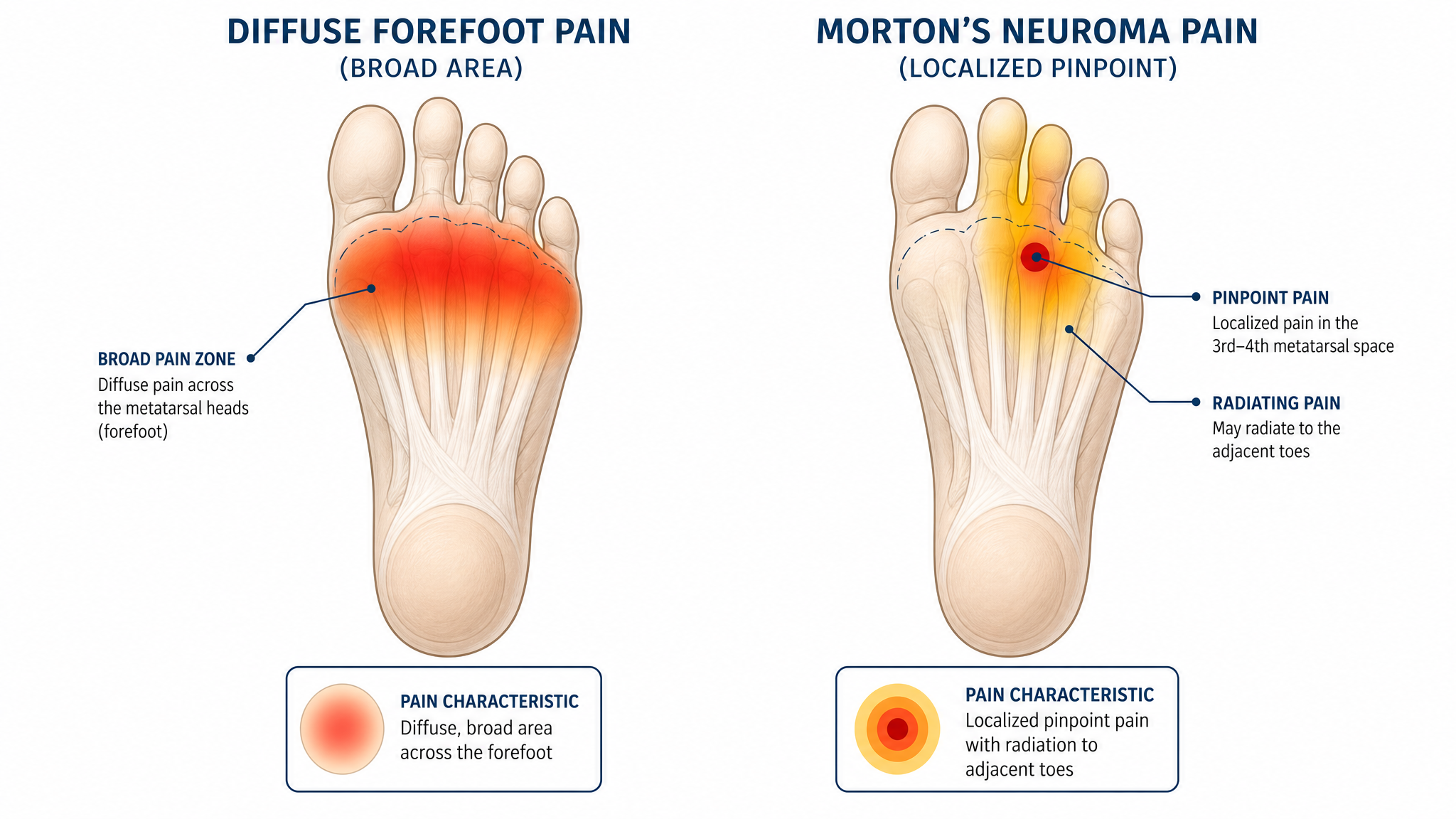
- The key difference: metatarsalgia causes broad aching pain; Morton’s neuroma causes sharp, electric, or tingling pain
- A simple squeeze test (Mulder’s sign) can help distinguish them at home
- Both conditions respond to metatarsal support insoles, but neuroma may also require wider toe boxes or nerve-specific treatments
- If you are unsure, seeing a podiatrist for a definitive diagnosis is always the safest approach
What Is Metatarsalgia?
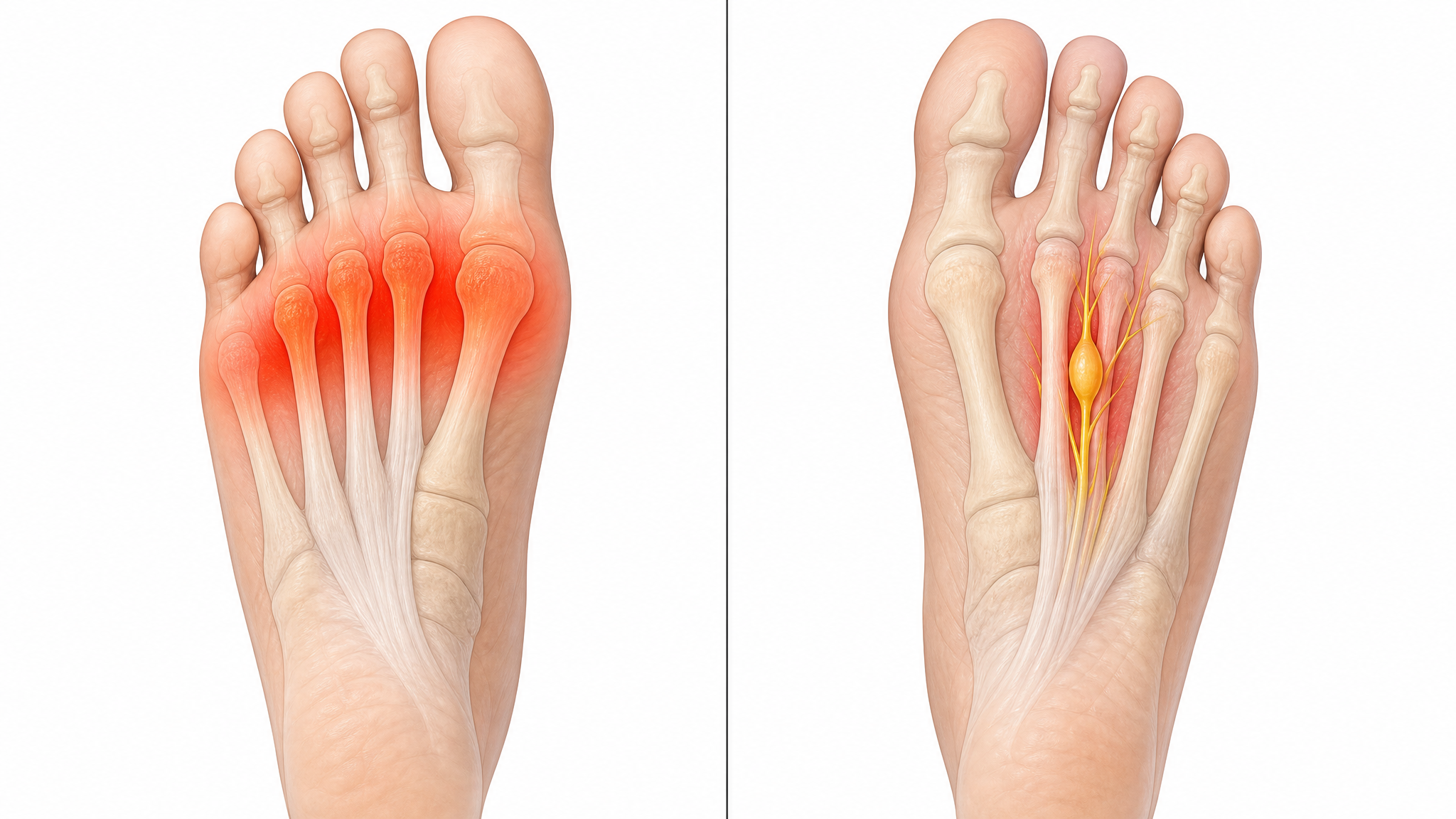
Metatarsalgia is a general term for pain and inflammation in the ball of the foot — specifically, the area where the five metatarsal bones meet the toes. It is not a single disease but a symptom complex with multiple possible causes.
The pain occurs when the metatarsal heads — the knuckle-like ends of these bones — experience excessive pressure. This can happen due to overuse, high-impact activity, poor footwear, foot structure abnormalities (high arches or flat feet), fat pad atrophy, or tight calf muscles.
Typical metatarsalgia sensation: A burning or aching pain across the ball of the foot that worsens with standing or walking. Many people describe it as feeling like “walking on pebbles” or having a stone in their shoe. The pain tends to develop gradually and eases with rest.
What Is Morton’s Neuroma?
Morton’s neuroma is a benign thickening of the nerve tissue that runs between the third and fourth toes (the interdigital nerve). Despite the name, it is not a true tumor — “neuroma” refers to the thickening that occurs when the nerve is repeatedly compressed or irritated.
The condition develops when the metatarsal bones pinch the nerve during walking, causing the nerve sheath to thicken over time. This is often aggravated by narrow shoes that squeeze the forefoot, high heels that increase forefoot pressure, or repetitive impact from running.
Typical Morton’s neuroma sensation: A sharp, shooting, or electric-shock pain in the ball of the foot, often radiating into the third and fourth toes. Many people report numbness or tingling in those toes. The pain may come and go and can be relieved by removing shoes and massaging the foot.
Key Differences at a Glance
| Factor | Metatarsalgia | Morton’s Neuroma |
|---|---|---|
| What it is | Inflammation of metatarsal bones | Thickening of the interdigital nerve |
| Pain type | Burning, aching, dull | Sharp, electric, shooting, tingling |
| Pain location | Across the ball of the foot | Between 3rd and 4th toes (most common) |
| Radiation | Stays in forefoot | Radiates into toes |
| Numbness/tingling | Uncommon | Common — in affected toes |
| Sensation | Walking on pebbles | Electric shock, “clicking” sensation |
| Aggravated by | Standing, walking, running | Narrow shoes, high heels, forefoot squeeze |
| Relieved by | Rest, supportive shoes | Removing shoes, foot massage |
The Home Test: Mulder’s Sign

There is a simple clinical test that podiatrists use to distinguish Morton’s neuroma from metatarsalgia — and you can do it at home.
How to perform Mulder’s test:
1. Sit with your foot resting on your opposite knee
2. Use one hand to squeeze the ball of your foot from side to side (compress the forefoot)
3. With your other hand, press firmly on the space between the third and fourth toes
Positive result (likely Morton’s neuroma): You feel a “click” or “pop” sensation under the ball of your foot, and this reproduces your pain or the electric-shock sensation
Negative result (likely metatarsalgia): Squeezing simply hurts across the entire forefoot without a clicking sensation, and the pain does not radiate into the toes
Quick Note
Mulder’s sign is a reliable diagnostic indicator, but a negative test does not completely rule out a small neuroma. If your symptoms suggest neuroma — sharp pain radiating into the toes — but the home test is negative, see a podiatrist. Ultrasound or MRI can confirm the diagnosis.
How the Conditions Are Connected
Metatarsalgia and Morton’s neuroma frequently coexist. The same factors that cause metatarsalgia — excessive forefoot pressure, narrow shoes, high impact — also contribute to nerve irritation. A person can have inflammation of the metatarsal heads (metatarsalgia) AND a thickened nerve (neuroma) simultaneously.
When they occur together, the metatarsalgia often develops first. As the forefoot remains inflamed, the constant pressure on the interdigital space irritates the nerve, eventually leading to neuroma formation. This is why treating forefoot pressure early — before nerve involvement develops — is important.
Treatment Differences

Treating Metatarsalgia
Metatarsalgia responds well to conservative treatment in most cases:
- Metatarsal support insoles — The primary treatment. A metatarsal dome lifts and separates the metatarsal heads, redistributing pressure
- Footwear changes — Wide toe boxes, rocker soles, and cushioned midsoles reduce forefoot pressure
- Stretching — Calf stretches reduce the forefoot loading that occurs with tight Achilles tendons
- Activity modification — Reducing high-impact activities during the acute phase allows inflammation to subside
Treating Morton’s Neuroma
Morton’s neuroma requires the same foundation plus additional nerve-specific measures:
- Metatarsal support insoles — Same as metatarsalgia; lifting the metatarsals takes pressure off the nerve
- Wide toe boxes — More critical for neuroma than metatarsalgia; the toes need room to spread and avoid compressing the nerve
- Avoiding high heels — Heels increase forefoot pressure and nerve compression
- Foot massage — Massaging the affected area can temporarily relieve nerve symptoms
- Professional treatment — If conservative measures fail: corticosteroid injections, alcohol sclerosing injections, or surgical nerve decompression
Important
If your forefoot pain has been diagnosed as “neuroma” and you have tried conservative treatment including wider shoes and metatarsal pads for 8 weeks without improvement, revisit your diagnosis. Predislocation syndrome (plantar plate injury) can mimic neuroma and requires different treatment. An ultrasound or MRI can confirm or rule out neuroma definitively.
When to See a Podiatrist
See a podiatrist for a definitive diagnosis if:
- You are unsure whether you have metatarsalgia or neuroma based on the home test
- Your pain persists after 6–8 weeks of conservative treatment
- You have significant numbness, tingling, or burning that radiates into your toes
- The pain is severe enough to alter your walking pattern
- You have diabetes or peripheral neuropathy
A podiatrist can perform ultrasound imaging to confirm the presence and size of a neuroma, prescribe custom orthotics with specific metatarsal accommodations, and offer in-office treatments if needed.
Can Insoles Help Both Conditions?
Yes. Metatarsal support insoles are effective for both metatarsalgia and Morton’s neuroma because they address the same underlying mechanical issue: excessive pressure on the forefoot. A correctly positioned metatarsal dome lifts the metatarsal heads, which:
- For metatarsalgia: Reduces direct pressure on the inflamed bones
- For Morton’s neuroma: Creates more space between the metatarsals, reducing nerve compression
The key is the same for both conditions: the metatarsal dome must be positioned just behind the metatarsal heads (approximately 1 cm behind the painful area), not directly under them.
The best flat feet and fallen arches insoles include models with built-in metatarsal support that work for both conditions, making them a good starting point regardless of your diagnosis.
Conclusion
Metatarsalgia and Morton’s neuroma are different conditions with different underlying causes, but they share a common solution: reducing forefoot pressure. If you have broad aching pain across the ball of your foot, you likely have metatarsalgia. If you have sharp, electric pain that shoots into your toes — especially between the third and fourth toes — Morton’s neuroma is more likely. Use Mulder’s sign as a home test, but see a podiatrist if you are unsure. In both cases, quality insoles with metatarsal support are the first and most effective step toward relief.
Not sure which condition you have?
Our orthotic insoles with metatarsal support provide relief for both metatarsalgia and Morton’s neuroma. Start with the right support today.
Free returns on all orders · 30-day money-back guarantee
Frequently Asked Questions
How do I know if I have metatarsalgia or Morton’s neuroma?
Use the location and quality of your pain as a guide. Aching pain across the entire ball of the foot suggests metatarsalgia. Sharp, electric, or tingling pain between the third and fourth toes that radiates into your toes suggests Morton’s neuroma. The Mulder’s sign squeeze test can help confirm.
Can you have both metatarsalgia and Morton’s neuroma at the same time?
Yes. The two conditions frequently coexist because the same factors — excessive forefoot pressure, narrow shoes, high impact — can cause both bone inflammation and nerve irritation. Treatment with metatarsal support insoles helps both conditions simultaneously.
What makes Morton’s neuroma worse?
Narrow shoes that squeeze the forefoot, high heels that increase forefoot pressure, and high-impact activities that compress the interdigital space all aggravate Morton’s neuroma. Removing your shoes and massaging the foot often provides temporary relief.
Is Morton’s neuroma serious?
Morton’s neuroma is not dangerous or life-threatening, but it can be painful and affect quality of life. It will not turn into cancer or cause permanent nerve damage in most cases. However, large neuromas or those left untreated for years can cause persistent symptoms that are harder to treat.
Do I need surgery for Morton’s neuroma?
Most cases of Morton’s neuroma do not require surgery. Conservative treatment — metatarsal pads, wide toe box shoes, activity modification — resolves symptoms in approximately 80% of cases. Surgery is typically considered only after 6–12 months of failed conservative treatment.
Can metatarsalgia turn into Morton’s neuroma?
Metatarsalgia does not directly turn into Morton’s neuroma, but the chronic forefoot pressure that causes metatarsalgia can also irritate the interdigital nerve over time, leading to neuroma formation. This is why treating forefoot pressure early is important.


