7 Causes of Forefoot Pain Your Doctor Might Be Missing
7 Causes of Forefoot Pain Your Doctor Might Be Missing
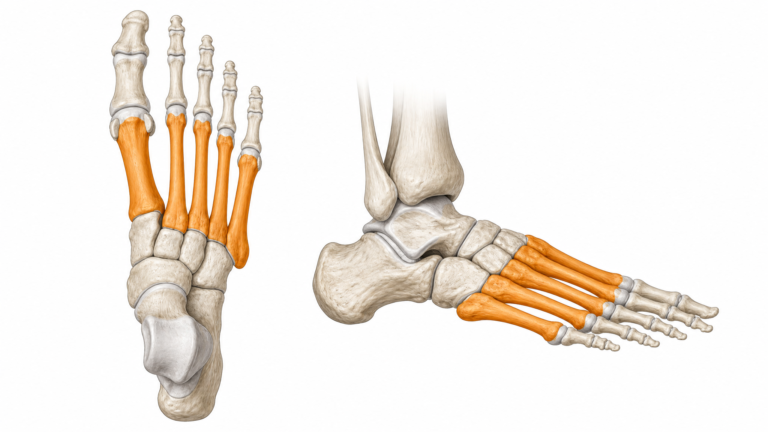
If you have been told you have “metatarsalgia” but your treatment is not working, there may be another explanation. The forefoot is a complex structure — five metatarsal bones, multiple nerves, tendons, ligaments, and small sesamoid bones — and several conditions can produce similar symptoms. Here are seven commonly overlooked or misdiagnosed causes of forefoot pain, how to recognize them, and what to do about each.
Key Takeaways
- “Metatarsalgia” is often a catch-all diagnosis that can mask more specific conditions
- Predislocation syndrome is frequently misdiagnosed as Morton’s neuroma — up to 30% of “neuroma” surgeries may be unnecessary
- Trigger points in the foot’s interosseous muscles can mimic nerve pain and are rarely considered in standard differentials
- Sesamoid disorders are underdiagnosed in athletes, with diagnostic delays averaging 6–12 months
- If your forefoot pain is not responding to treatment, consider asking your doctor specifically about these conditions
1. Predislocation Syndrome (Plantar Plate Injury)
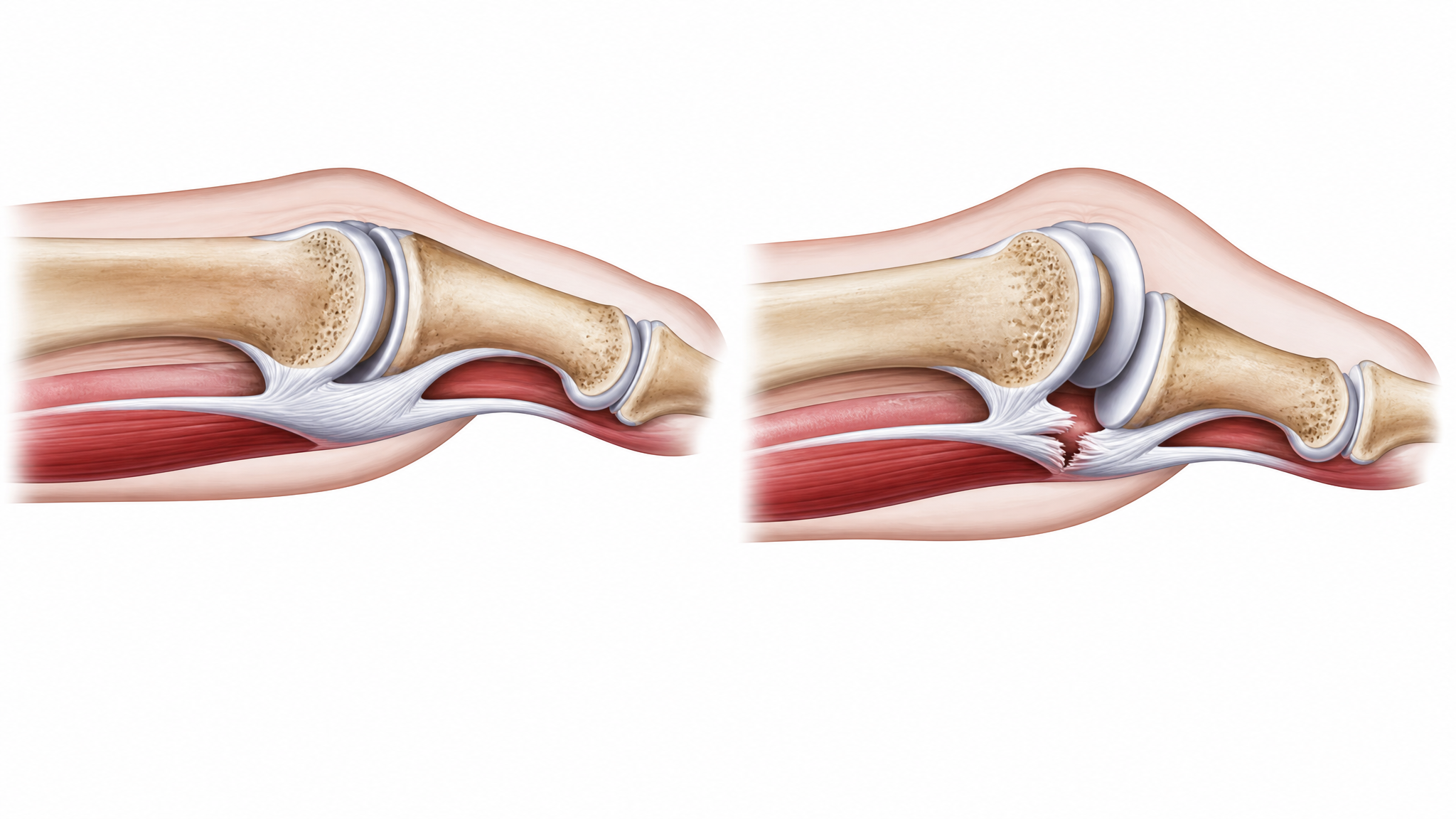
What it is. Predislocation syndrome is a progressive injury to the plantar plate — the thick ligamentous structure under the metatarsophalangeal joints that stabilizes your toes. When the plantar plate becomes attenuated or tears, the toe starts to drift out of alignment.
Why it is missed. Predislocation syndrome is described in podiatric literature as “frequently unrecognized or misdiagnosed.” The early symptoms — bruise-like ache under the ball of the foot, mild swelling at the base of the toe — closely mimic metatarsalgia or a mild neuroma. Many patients undergo neuroma surgery that does not help because the actual problem is the plantar plate.
How to recognize it. The hallmark sign is a “vertical stress test” — if your doctor can lift your toe upward and reproduce your ball-of-foot pain, the plantar plate is likely involved. As the condition progresses, the affected toe (usually the second toe) starts to cross over the big toe. In its earliest stages, you may notice your second toe sitting slightly higher than normal when viewed from the side.
What to do. Plantar plate injuries require specific treatment: taping to stabilize the toe, stiff-soled shoes or carbon plate inserts to limit MPJ flexion, and in advanced cases, surgical repair. Standard metatarsal pads may help symptoms but will not address the underlying instability.
2. Interosseous Trigger Points (Myofascial Pain Syndrome)
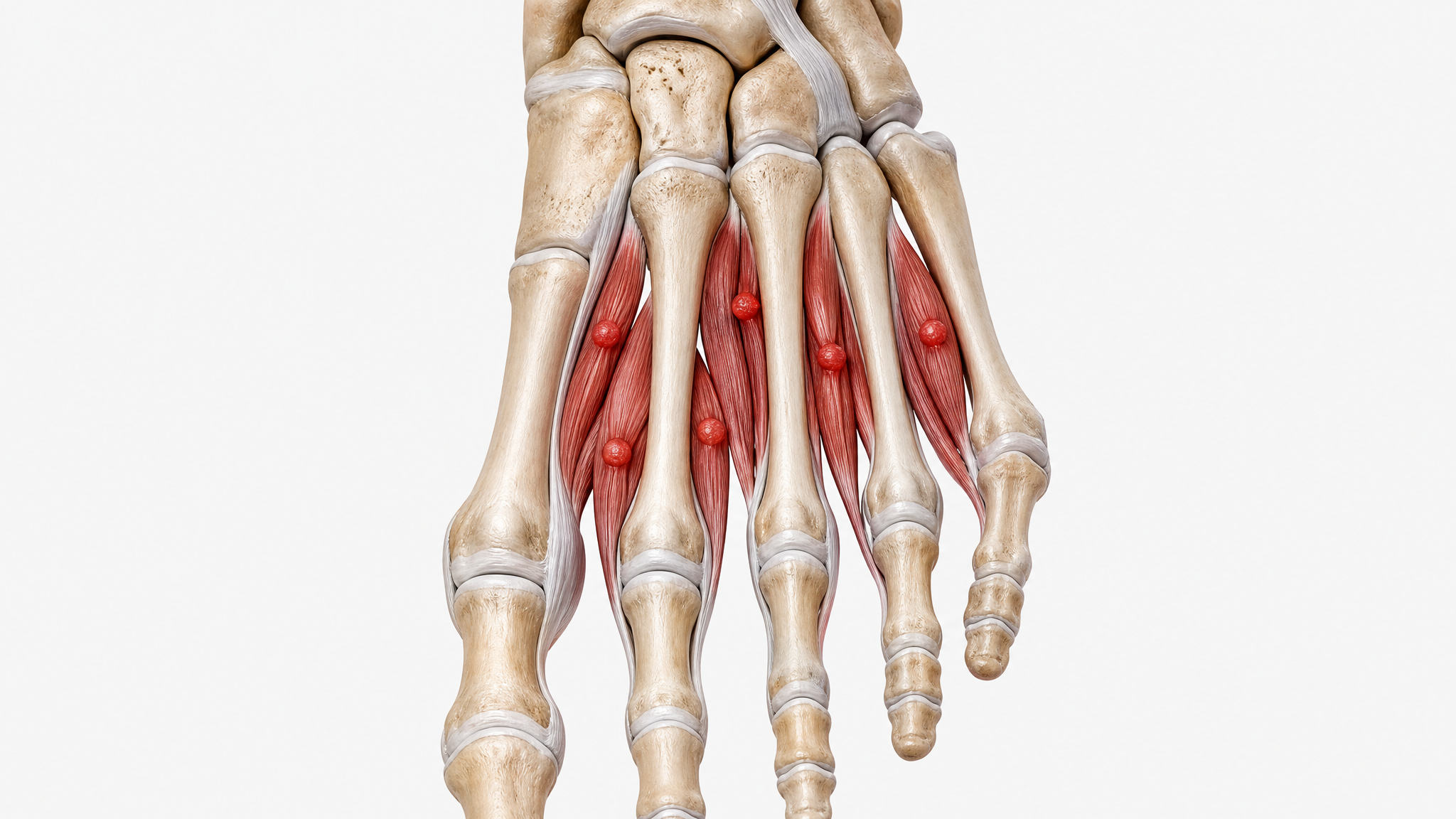
What it is. The interosseous muscles lie between the metatarsal bones and help control toe movement. Like any muscle, they can develop trigger points — hyperirritable knots that refer pain to other areas. A 2024 study in Ultrasonography explicitly identified these trigger points as an “overlooked cause of metatarsalgia.”
Why it is missed. Trigger points do not show up on X-ray, ultrasound, or MRI unless specifically looked for. The standard diagnostic workup for forefoot pain — physical exam, X-ray, maybe MRI — does not include manual palpation for myofascial trigger points unless the practitioner is specifically trained in myofascial diagnosis.
How to recognize it. The pain is often described as a deep ache between specific metatarsals that can radiate toward the toes or up the foot. Unlike metatarsalgia (which hurts when you press on the bone), trigger point pain is reproduced by pressing into the muscle belly between the bones.
What to do. Treatment includes targeted massage, trigger point release, dry needling, or shockwave therapy performed by a qualified practitioner. Foam rolling the foot with a lacrosse ball can provide temporary relief, but professional myofascial treatment is often needed for lasting resolution.
3. Sesamoid Avascular Necrosis (AVN)
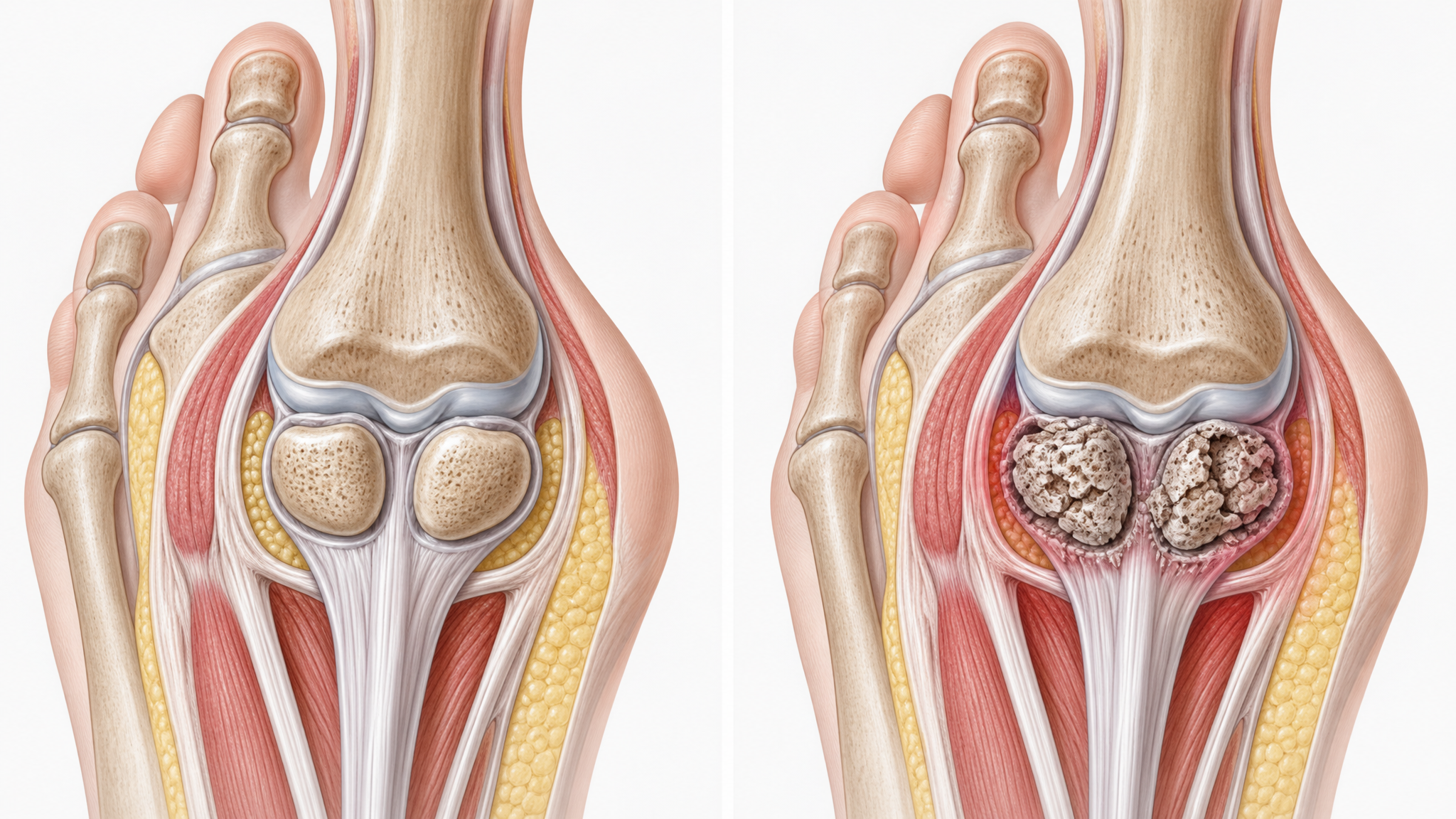
What it is. The sesamoid bones are two tiny pea-shaped bones embedded in the tendon under the big toe joint. They help with leverage during walking and running. Avascular necrosis occurs when the blood supply to a sesamoid bone is disrupted, causing the bone tissue to die.
Why it is missed. AVN of the sesamoids is described in the 2025 literature as an “overlooked cause of forefoot pain in athletes” with diagnostic delays averaging 6–12 months. Standard X-rays may appear normal in the early stages — the bone death does not show up until the bone collapses, which can take months. Even then, it can be mistaken for sesamoiditis (simple inflammation).
How to recognize it. Pain is specifically under the big toe joint (the hallux), not the general ball of the foot. It worsens with push-off during walking or running and does not improve with rest alone. There may be localized tenderness directly over one sesamoid bone rather than the other.
What to do. Sesamoid AVN requires an MRI for definitive diagnosis. Treatment ranges from activity modification and custom orthotics with sesamoid cutouts to immobilization and, in advanced cases, surgical removal of the affected sesamoid.
4. Lesser Metatarsal Sesamoids (Accessory Bones)
What it is. Some people are born with extra sesamoid bones near the lesser metatarsals (the second through fifth toes). These accessory bones are anatomical variants — they are not supposed to be there, and when present, they can cause pain by rubbing against adjacent bones or tendons.
Why it is missed. Accessory sesamoids are “underreported in radiology and podiatry literature.” Most radiologists and podiatrists are trained to look for the two standard sesamoids under the big toe. Additional sesamoids elsewhere in the forefoot are often dismissed as normal variants or simply not noticed on imaging.
How to recognize it. Pain that occurs at a specific point in the forefoot — not the general ball of the foot — and is reproducible by pressing on that exact spot. The pain may be aggravated by certain shoe types but not others, depending on where the extra bone contacts the shoe.
What to do. Ultrasound or MRI can identify accessory sesamoids. Treatment is the same as for sesamoiditis: padding to offload the area, stiff-soled shoes, and in persistent cases, surgical excision.
Quick Note
If your forefoot pain does not respond to standard metatarsalgia treatment after 8 weeks, ask your doctor specifically about these conditions. “Metatarsalgia” is a symptom description, not a diagnosis — and treating the wrong condition wastes time and money.
5. Trigger Toe (Flexor Pulley Injury)
What it is. “Trigger toe” is a lesser-known condition where the flexor pulley system in the toes — the same type of structure that causes trigger finger in the hand — becomes inflamed and catches during movement. It has been described in recent research as a “previously undescribed” and “more common than recognized” cause of forefoot pain.
Why it is missed. The flexor pulley system in the toes was not well described in anatomy literature until recently. Most clinicians do not know to look for it. Patients with trigger toe are often told they have metatarsalgia or a neuroma because the clicking sensation under the foot is mistaken for Mulder’s sign.
How to recognize it. The key sign is a catching or clicking sensation under the ball of the foot when you curl your toes. Unlike neuroma (where the click is felt with side-to-side compression), trigger toe produces a click when you actively curl your toes downward.
What to do. Trigger toe often responds to physical therapy focusing on toe flexor stretching and strengthening. In persistent cases, corticosteroid injection around the pulley or surgical release may be needed.
6. Schwannoma (Nerve Sheath Tumor)
What it is. A schwannoma is a benign tumor of the nerve sheath — the protective covering around a nerve. When it occurs on the medial plantar nerve or one of its branches in the foot, it produces symptoms that closely mimic metatarsalgia or Morton’s neuroma.
Why it is missed. Schwannomas of the foot are rare, and the standard workup for forefoot pain does not include imaging that would detect them. Case reports document patients treated for metatarsalgia or neuroma for months to years before imaging finally revealed a schwannoma.
How to recognize it. Unlike typical metatarsalgia (which is broad and aching), schwannoma pain tends to follow the distribution of a specific nerve. It may produce a “Tinel’s sign” — tapping over the affected area reproduces a tingling or electric sensation down the nerve pathway.
What to do. MRI can identify schwannomas. Treatment is surgical excision, which usually resolves symptoms completely as the tumor is benign and well-encapsulated.
7. Capsulitis of the Lesser MPJ

What it is. Capsulitis is inflammation of the joint capsule surrounding the metatarsophalangeal joints (where your toes meet your foot). It is most common at the second MPJ but can affect any of the lesser toes.
Why it is missed. Capsulitis is often labeled as “metatarsalgia” because the pain is in the same location. The distinction matters because capsulitis involves the joint capsule specifically, not the bone, and may require different treatment including joint protection and anti-inflammatory measures.
How to recognize it. Capsulitis produces pain at the base of a specific toe (usually the second), with swelling and a sensation that the toe feels “loose” or unstable. There is often a positive “drawer sign” — your doctor can shift the toe slightly forward and backward more than normal, indicating the joint capsule is lax.
What to do. Treatment includes joint taping to stabilize the MPJ, stiff-soled shoes or carbon plates to limit MPJ flexion, and anti-inflammatory measures. If caught early, capsulitis resolves well with conservative treatment. If allowed to progress, it can lead to predislocation syndrome and chronic instability.
Conclusion
Persistent forefoot pain that does not respond to standard metatarsalgia treatment warrants a closer look. The conditions above are not rare — they are simply overlooked because “metatarsalgia” has become a catch-all diagnosis. If your treatment is not working, ask your doctor about these specific possibilities. In the meantime, quality insoles with metatarsal support will help manage symptoms for most forefoot conditions while you pursue the correct diagnosis.
Support your feet while you find the right diagnosis.
Our orthotic insoles provide broad forefoot support that helps manage symptoms across multiple conditions.
Free returns on all orders · 30-day money-back guarantee
Frequently Asked Questions
What is the most commonly missed cause of forefoot pain?
Predislocation syndrome (plantar plate injury) is one of the most commonly missed causes. It mimics Morton’s neuroma and metatarsalgia but requires different treatment. Some estimates suggest up to 30% of neuroma surgeries may be performed on patients who actually have plantar plate injuries.
How do I know if my doctor has the right diagnosis?
If your “metatarsalgia” treatment is not working after 8 weeks, ask for a more specific diagnosis. A good podiatrist should be able to perform tests — vertical stress test, drawer sign, Mulder’s sign, trigger point palpation — to narrow down the cause.
Can trigger points cause forefoot pain?
Yes. Myofascial trigger points in the interosseous muscles between the metatarsals can refer pain that feels like metatarsalgia or nerve pain. This is documented in recent 2024 medical literature as an “overlooked” cause.
What imaging is needed for undiagnosed forefoot pain?
Start with weight-bearing X-rays to assess bone alignment. If the X-rays are normal but pain persists, MRI is the most useful next step — it can show soft tissue injuries (plantar plate, capsule), nerve thickening (neuroma), sesamoid AVN, and schwannomas that X-rays miss. Ultrasound is another option for neuroma diagnosis.
When should I consider a second opinion on forefoot pain?
If you have seen one doctor, received a treatment plan, followed it for 8 weeks without improvement, and no imaging has been done, consider a second opinion. An accurate diagnosis of forefoot pain often requires specific clinical tests and imaging that not all practitioners perform routinely.