
Best Running Insoles for Achilles Tendonitis
The best running insoles for Achilles tendonitis combine semi-rigid arch support with a deep heel cup, not just cushioning. Most runners reach for a soft gel insole and wonder why the pain keeps coming back. Cushioning alone doesn’t address the mechanical problem driving the injury.
Key Takeaways
- Arch support controls overpronation, which is the primary mechanical driver of Achilles tendonitis in runners
- Insertional tendonitis (pain at the heel bone) needs heel cushioning and a slight lift; mid-portion tendonitis (2–6cm above the heel) needs arch support to stop rotational twisting
- Running shoes already have 8–12mm of heel drop; adding a thick insole can push total heel elevation too high and change your gait
- Look for a low-profile insole (under 5mm total thickness), deep heel cup (12mm+), and moisture-wicking top cover
- You do not need to stop running, reducing mileage 40–50% and avoiding hills is more effective than complete rest
Why Running Makes Achilles Tendonitis Different
Runners put 3–4x their body weight through the Achilles tendon with every stride. That load is manageable when foot mechanics are sound. When they aren’t, specifically when the foot overpronates and rolls inward, the tendon twists slightly with each footfall. Over thousands of steps per run, that rotational stress accumulates into the inflammation and micro-tearing that defines tendonitis.
The challenge for runners is that the fix has to work inside a running shoe, not a dress shoe or work boot. Running shoes are already engineered with heel drop, cushioning stacks, and specific geometry. An insole that works well in a casual shoe can throw off running mechanics entirely if it raises the heel too high or adds too much bulk.
That’s why the insole features that matter for runners are different from what most general guides recommend.
Insertional vs. Mid-Portion: Why the Location Changes Everything
This distinction is the most important thing to understand before choosing an insole, and it’s one most articles skip entirely.
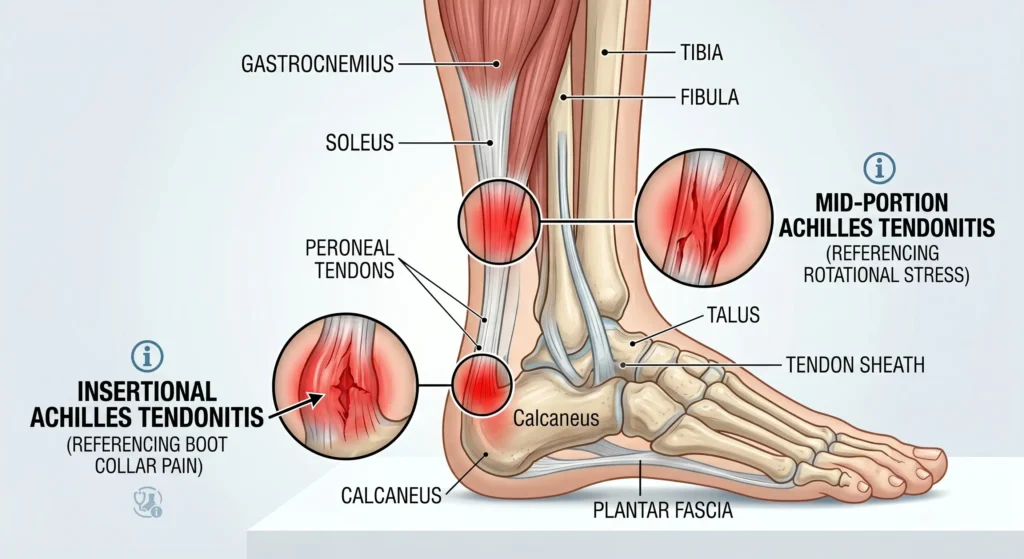
Insertional Achilles Tendonitis
Insertional tendonitis affects the point where the tendon attaches to the heel bone. Pain sits right at the back of the heel, often with a visible bump (Haglund’s deformity). It’s more common in runners who do a lot of hill work or who wear shoes with a low heel drop.
For insertional tendonitis, the goal is to reduce compression and tension at the attachment point. A slight heel lift (6–8mm) reduces the angle of pull on the tendon. Cushioning at the heel absorbs impact. Critically, avoid heel cups that have a hard rim pressing directly on the insertion, that contact point can aggravate the condition significantly.
Mid-Portion Achilles Tendonitis
Mid-portion tendonitis affects the tendon 2–6cm above the heel bone. This is the more common presentation in distance runners. The tendon here has a relatively poor blood supply, which is why it heals slowly and why chronic cases are so frustrating.
The primary driver in runners is overpronation. When the foot rolls inward, the Achilles tendon twists. Arch support insoles correct that inward roll at the source, reducing the rotational load on the tendon with every stride. A heel lift alone does almost nothing for mid-portion tendonitis.
Good to Know
Not sure which type you have? Press firmly along the back of your heel. If the most tender spot is right at the bone, that’s insertional. If it’s 2–6cm above the heel in the tendon itself, that’s mid-portion. Many runners have both, which is why a combination insole, arch support plus moderate heel cushioning, tends to work best.
The Features That Actually Matter in a Running Insole
Not all insole features translate to running. Here’s what to prioritize and why.
Semi-Rigid Arch Support
Soft foam arch support compresses under load and provides little mechanical correction. You need a semi-rigid shell, typically polypropylene or a firm EVA, that holds its shape through the push-off phase of your stride. This is what actually controls overpronation.
Full-rigid orthotics can be too stiff for running, reducing the natural energy return of your foot. Semi-rigid is the sweet spot: enough structure to correct mechanics, enough flex to work with your gait.
Deep Heel Cup (12mm Minimum)
A deep heel cup cradles the fat pad under your heel and keeps it centered under the calcaneus. This improves shock absorption and stabilizes the rearfoot, reducing the side-to-side motion that contributes to tendon stress. For running, aim for at least 12mm of heel cup depth.
Low-Profile Design
This is where most insoles fail runners. Your running shoe already has a built-in midsole and heel drop. Adding a thick aftermarket insole raises your heel further, potentially pushing total heel elevation past the point where your Achilles is comfortable. It can also make the shoe fit too tight across the midfoot.
Look for insoles under 5mm total thickness at the forefoot. Many running-specific insoles are designed with this constraint in mind; general-purpose insoles often are not.
Moisture-Wicking Top Cover
Runners sweat. A top cover that traps moisture creates friction, blisters, and odor. Look for a fabric or perforated top layer that moves moisture away from the foot. This is a comfort feature, but it also affects how long the insole lasts.
Runner Profiles: Which Insole Type Fits You
Different runners have different needs. Here’s how to match insole type to your situation.
The Overpronator with Mid-Portion Pain
This is the most common runner profile presenting with Achilles tendonitis. The foot rolls inward excessively, the tendon twists, and pain develops in the mid-tendon. The fix is a firm arch support insole that controls that inward roll.
Look for arch support insoles with a semi-rigid shell, deep heel cup, and low-profile forefoot. If you also have flat feet, insoles for flat feet and overpronation are specifically designed for this combination.
The Neutral Runner with Insertional Pain
Neutral runners, those without significant overpronation, who develop insertional tendonitis usually have a different problem: too much heel impact, often from running downhill or in low-drop shoes. The fix here is heel cushioning with a moderate lift.
Silicone gel insoles work well for this profile. They absorb impact effectively and provide a slight heel elevation without adding significant bulk. Avoid heel cups with a hard posterior rim that contacts the insertion point directly.
The High-Mileage Runner with Both Types
High-mileage runners often present with a combination of insertional and mid-portion symptoms. The tendon is under chronic load, and both the insertion and the mid-substance are affected. This profile benefits from a combination insole: semi-rigid arch support for mechanical correction, plus moderate heel cushioning for impact absorption.
A full-length insole with a firm arch shell and a cushioned heel zone is the right choice here. Pair it with a review of your weekly mileage, if you’re running more than 40 miles per week with Achilles symptoms, the insole alone won’t be enough.
What to Avoid
Some common choices make Achilles tendonitis worse in runners.
Thick Cushioning Insoles Without Arch Support
Soft, thick insoles feel comfortable at first. But they compress under load, provide no mechanical correction, and often raise the heel too high inside the shoe. Runners with overpronation who use soft cushioning insoles frequently report that symptoms worsen over time.
Heel Cups That Press on the Insertion
Hard-rimmed heel cups are designed to cradle the heel, but if the rim contacts the Achilles insertion directly, it creates a pressure point that aggravates insertional tendonitis. If you have insertional pain, choose an insole with a smooth, open heel cup or a U-shaped cutout at the posterior rim.
Insoles That Don’t Fit Your Shoe
An insole that’s too thick for your running shoe will compress the midfoot, alter your foot position, and change your gait mechanics in unpredictable ways. Always check the fit with your running shoes before committing to an insole.
Important
If you feel a sudden sharp pop at the back of your heel followed by an inability to push off your foot, stop running immediately. This can indicate an Achilles tendon rupture, which is a serious injury requiring urgent medical evaluation. Do not attempt to walk it off or continue your run. Seek medical attention the same day.
Runner Stories: What Recovery Actually Looks Like
Marcus, 38, Marathon Trainer
Marcus had been training for his third marathon when mid-portion Achilles pain forced him to cut his long runs short. He’d tried a gel heel cup with no improvement. The problem was overpronation, his left foot rolled inward significantly, and the gel cup did nothing to address it.
He switched to a semi-rigid arch support insole and reduced his weekly mileage from 55 to 30 miles, cutting out all hill repeats and tempo work. Within three weeks the morning stiffness had eased. At eight weeks he was back to full training. He finished his marathon at week 14, two weeks ahead of his original timeline.
Priya, 31, Recreational Runner
Priya ran four days a week and developed insertional Achilles pain after switching to a minimalist shoe with a 4mm heel drop. The low drop increased the load on her Achilles insertion, and the hard heel counter of the new shoe pressed directly on the tender spot.
She returned to her previous shoes with an 8mm drop and added shock-absorbing insoles with a smooth heel cup. She also started eccentric heel drops, the Alfredson protocol, three times per week. Pain resolved at six weeks. She now uses the insoles in all her running shoes as a preventive measure.
David, 45, Trail Runner
David had chronic Achilles issues for two years before understanding the insertional vs. mid-portion distinction. His pain was mid-tendon, but he’d been using heel lifts based on advice from a running forum. The lifts helped slightly but never resolved the problem.
A gait analysis confirmed significant overpronation. He switched to insoles for Achilles tendonitis with a firm arch shell and reduced his trail running to flat routes only for eight weeks. The combination of mechanical correction and load management resolved symptoms that two years of heel lifts had failed to fix.
Load Management: You Don’t Have to Stop Running
Complete rest is rarely the right answer for Achilles tendonitis. The tendon needs load to heal, it’s the type and volume of load that matters.
The evidence-based approach is load management: reduce total mileage by 40–50%, eliminate hills and speed work, and keep easy running on flat surfaces. This maintains tendon conditioning while removing the high-stress activities that drive inflammation.
Pair load management with eccentric heel drops (the Alfredson protocol): stand on a step, rise on both feet, then lower slowly on the affected foot only. Three sets of 15 repetitions, twice daily. This is the most evidence-supported rehabilitation exercise for Achilles tendonitis and works alongside insoles, not instead of them.
Return-to-full-training timeline with proper management is typically 6–12 weeks. Runners who try to push through without reducing load often extend that timeline to 6 months or longer.
If you notice Achilles tendon sounds during running, creaking, clicking, or popping, that’s worth monitoring. Occasional sounds without pain are usually benign, but persistent sounds with pain warrant a medical evaluation.
How to Choose the Right Insole for Your Running Shoes
The insole has to work with your specific shoe, not just your foot. Here’s a practical approach.
Check Your Shoe’s Existing Insole
Remove the factory insole and measure its thickness at the heel and forefoot. This tells you how much space you have. Most running shoes have 4–6mm of removable insole. An aftermarket insole in the same thickness range will fit without changing the shoe’s geometry significantly.
Match Insole Stiffness to Your Arch Type
Low arches (flat feet) need firmer arch support to prevent collapse. High arches need more cushioning and a shallower arch profile. Neutral arches can use either, but semi-rigid support is still preferable to soft foam for Achilles tendonitis management.
Test the Fit Before Running
Walk in the insoles for 30–60 minutes before your first run. Check that the arch support sits under your arch (not behind it), the heel cup cradles your heel without pressing on the Achilles insertion, and the forefoot isn’t elevated uncomfortably. If anything feels off, the insole isn’t the right fit for your foot-shoe combination.
The Complete Recovery Approach
Insoles are one part of a multi-component recovery plan. The runners who recover fastest combine all of these:
- Insoles: Semi-rigid arch support to correct overpronation, heel cushioning to reduce impact
- Load management: 40–50% mileage reduction, no hills or speed work
- Eccentric exercises: Alfredson protocol, twice daily
- Footwear review: Adequate heel drop (8–12mm), no worn-out midsoles
- Patience: 6–12 weeks is realistic; 2–3 weeks is not
The best insoles for Achilles tendonitis address the mechanical root cause. Everything else in this list supports the healing environment. None of these elements works as well in isolation as they do together.
Find the Right Insole for Your Running Style
RoamingFeet’s arch support insoles are designed for runners who overpronate, the most common mechanical driver of Achilles tendonitis. Semi-rigid support, deep heel cup, low-profile fit for running shoes.
Shop Arch Support Insoles →Free shipping on $50+ · Free returns on all orders
Frequently Asked Questions
Do insoles actually help Achilles tendonitis in runners?
Yes, but the type of insole matters. Semi-rigid arch support insoles reduce overpronation, which is the primary mechanical driver of Achilles tendonitis in most runners. Soft cushioning insoles without arch support provide comfort but don’t address the root cause. Runners with mid-portion tendonitis see the most benefit from arch support; those with insertional tendonitis benefit more from heel cushioning with a moderate lift.
Can I keep running with Achilles tendonitis if I use insoles?
In most cases, yes, with modifications. Reduce your mileage by 40–50%, eliminate hills and speed work, and stick to flat, easy running. Insoles help manage the mechanical load, but they don’t eliminate it entirely. Complete rest is rarely necessary and can actually slow recovery by reducing the tendon’s conditioning stimulus.
How long before insoles reduce Achilles tendonitis pain?
Most runners notice reduced pain within 2–4 weeks of consistent insole use combined with load management. Full resolution typically takes 6–12 weeks. If pain hasn’t improved after 4–6 weeks of proper insole use and load management, a physiotherapy assessment is worthwhile to rule out other contributing factors.
Will any insole fit in my running shoes?
Not all insoles are compatible with running shoes. Running shoes have a specific geometry and heel drop that aftermarket insoles can disrupt if they’re too thick. Look for low-profile insoles under 5mm at the forefoot. Always remove the factory insole before inserting an aftermarket one, and check the fit before your first run.
What’s the difference between insoles and custom orthotics for Achilles tendonitis?
Custom orthotics are individually molded to your foot and can address specific biomechanical issues with greater precision. They’re also significantly more expensive, typically $300–$600 versus $20–$60 for quality OTC insoles. For most runners with Achilles tendonitis, a well-chosen semi-rigid OTC insole provides comparable mechanical correction. Custom orthotics are worth considering if OTC options haven’t resolved symptoms after 8–12 weeks.




