Metatarsalgia in Runners: Causes, Prevention & Treatment
Metatarsalgia in Runners: Causes, Prevention & Treatment
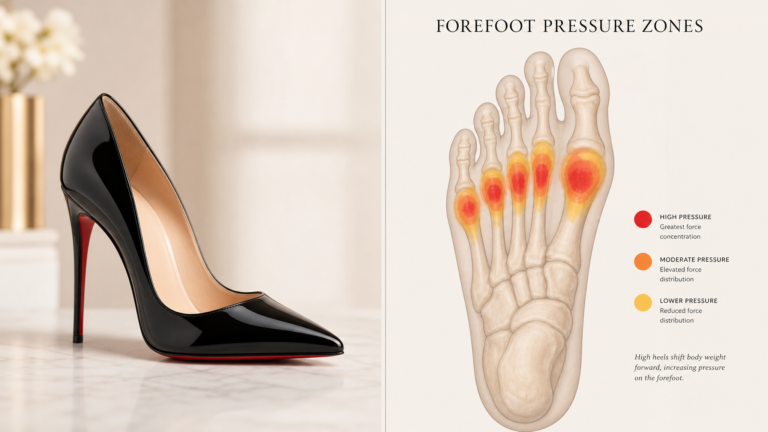
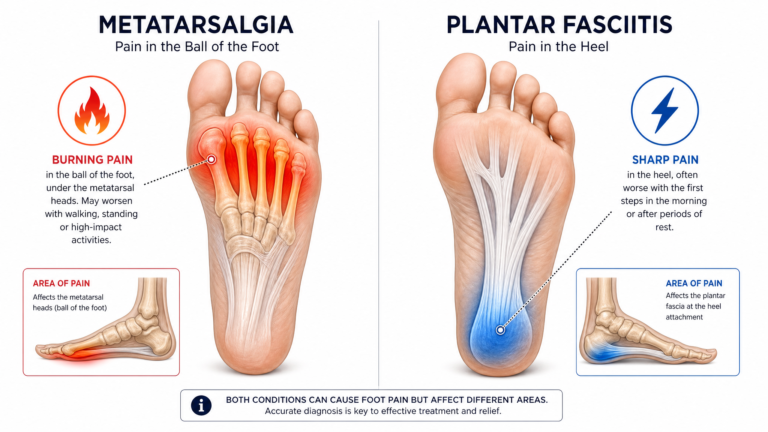
If you are a runner with metatarsalgia, you know the frustration: that burning ache across the ball of your foot that starts a few miles into a run and forces you to slow down or stop. Running places 3–5 times your body weight on each foot with every stride, and the forefoot absorbs a disproportionate share of that impact. This guide covers why runners are prone to metatarsalgia, how to prevent it, and how to treat it so you can get back to running pain-free.
Key Takeaways
- Running multiplies forefoot load by 3–5 times body weight, making metatarsalgia one of the most common running injuries
- The leading causes in runners: worn-out shoes, sudden mileage increases, tight calves, and running form issues
- Most running-related metatarsalgia resolves with rest, insoles, and gradual return to running
- Prevention is more effective than treatment — replace shoes on schedule, increase mileage gradually, and maintain calf flexibility
- Return to running should follow a structured progression: pain-free walking for 2 weeks, then walk-run intervals, then full running
Why Runners Get Metatarsalgia
Running creates repetitive, high-magnitude loading on the forefoot. Unlike walking (where the heel strikes first and weight transitions smoothly to the forefoot), running involves higher impact forces and a longer proportion of each stride spent on the forefoot.
Several factors specific to running contribute to metatarsalgia:
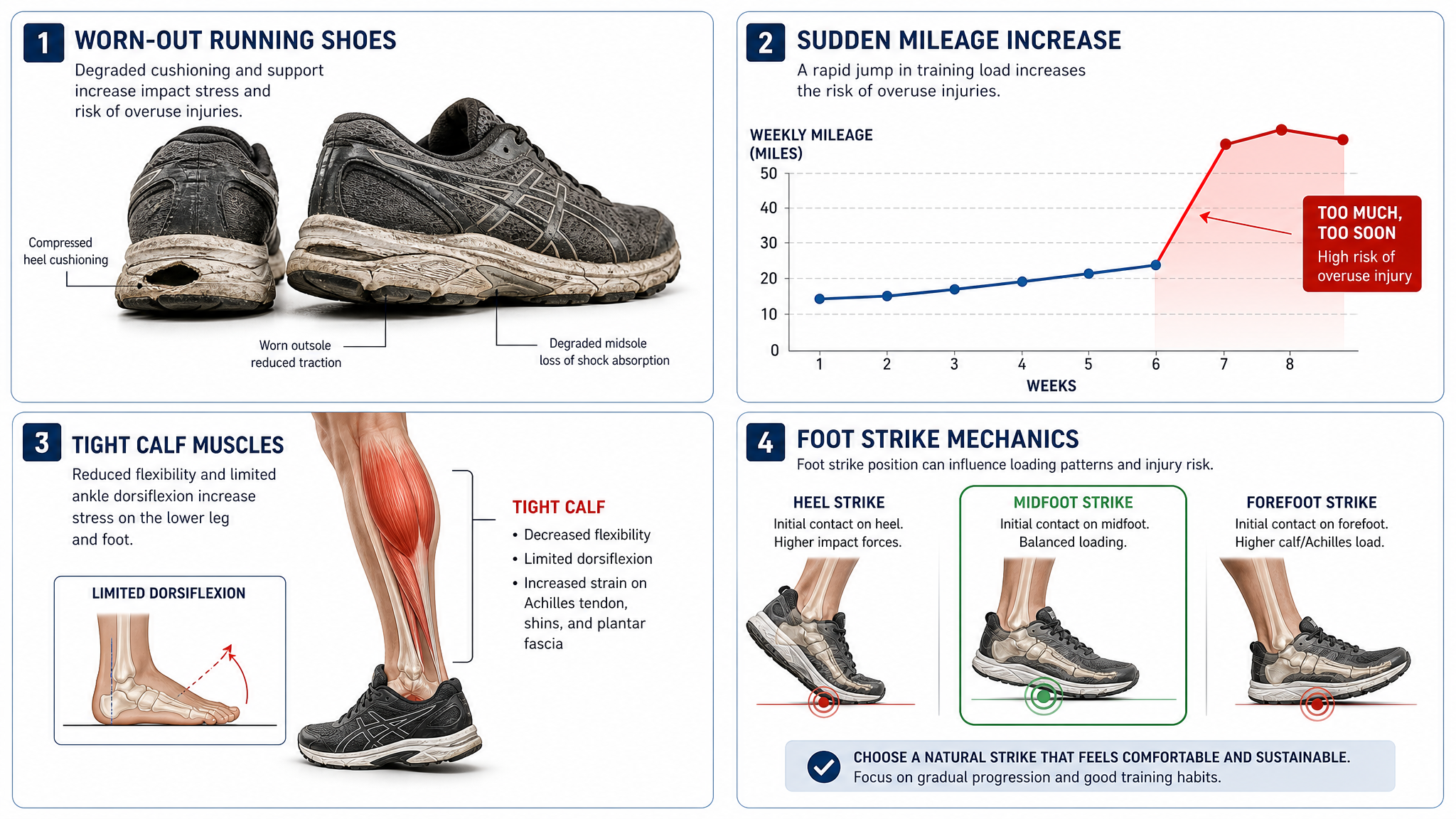
Worn-out running shoes. Running shoes lose their cushioning after 300–500 miles. Continuing to run in worn shoes increases the impact transmitted to the metatarsal heads with every stride. This is the most common cause of running-related metatarsalgia.
Sudden mileage increases. The “too much, too soon” principle applies directly to metatarsalgia. Increasing weekly mileage by more than 10% does not give the metatarsal heads time to adapt to the increased load.
Tight calves in runners. Runners tend to have tight calves due to the repetitive plantar flexion involved in running. Tight calves reduce ankle dorsiflexion, forcing more load onto the forefoot.
Forefoot or midfoot striking. Runners who land on their forefoot or midfoot place significantly more load on the metatarsal heads than heel strikers. While forefoot striking is not inherently bad, a sudden switch to this gait pattern can overload the forefoot.
Running on hard surfaces. Concrete and asphalt transmit more impact to the forefoot than softer surfaces like trails, grass, or tracks.
Prevention Strategies

Replace Shoes on Schedule
This is the single most effective prevention measure. Running shoes lose approximately 30–40% of their cushioning before the outsole shows visible wear. Replace your running shoes every 300–500 miles, depending on your weight, running surface, and gait. If you are heavier or run primarily on hard surfaces, replace closer to 300 miles.
Follow the 10% Rule
Increase your weekly mileage by no more than 10% per week. This gives your bones, tendons, and ligaments time to adapt to the increased load. Sudden jumps in mileage are one of the most common triggers of metatarsalgia in runners.
Maintain Calf Flexibility
Incorporate calf stretching into your post-run routine. Tight calves are a primary contributor to forefoot pressure, and runners are especially prone to calf tightness. Stretch both the straight-leg (gastrocnemius) and bent-knee (soleus) versions for 30 seconds each, 3 repetitions per side.
Strengthen Foot Intrinsics
Strong intrinsic foot muscles help distribute force across the foot and reduce the burden on the metatarsal heads. Add towel curls, marble pickups, and toe spreading/doming to your cross-training routine 2–3 times per week.
Vary Your Running Surfaces
Alternate between hard surfaces (roads, sidewalks) and softer surfaces (trails, grass, track). Softer surfaces reduce the impact transmitted to the forefoot. If you run primarily on concrete, aim to mix in at least one softer-surface run per week.
Treatment for Runners
Immediate Steps (Acute Phase)
When you first notice forefoot pain during or after running:
- Stop running for 3–7 days. Complete rest from running allows acute inflammation to subside.
- Ice the forefoot. Apply ice for 15 minutes, 2–3 times per day. A frozen water bottle rolled under the foot combines ice with gentle massage.
- Switch to low-impact cross-training. Swim, cycle, or use the elliptical to maintain fitness without loading the forefoot.
- Start wearing supportive insoles immediately. The best insoles for ball of foot pain provide immediate pressure relief with a metatarsal dome.
Recovery Phase

Once you can walk pain-free for several days, begin a structured return to running:
Week 1: Walk-run intervals. Walk 4 minutes, run 1 minute. Repeat 4–5 times. Run at a conversational pace. Do this every other day.
Week 2: Increase run intervals. Walk 3 minutes, run 2 minutes. Repeat 4–5 times. Continue every other day.
Week 3: Build run time. Walk 2 minutes, run 4 minutes. Repeat 4–5 times. You should be running 3–4 times per week by this point.
Week 4: Return to continuous running. If pain-free during all walk-run intervals, attempt a continuous 20-minute run at an easy pace. If pain-free, gradually increase duration by 10% per week.
When to See a Podiatrist
See a podiatrist if:
– You cannot walk pain-free after 2 weeks of rest and conservative treatment
– The pain returns each time you try to resume running
– You have a tender spot on one specific metatarsal (possible stress fracture)
– There is swelling or bruising in the forefoot
Important
Metatarsal stress fractures are a risk for runners with persistent forefoot pain. If your pain is focused on a single metatarsal bone rather than across the forefoot, and it hurts to press on that specific spot, stop running and see a podiatrist for an X-ray before resuming any impact activity.
Choosing Running Shoes for Metatarsalgia
The right running shoes are critical for both prevention and recovery. Many runners specifically search for metatarsalgia running shoes — footwear designed to minimize forefoot impact while maintaining performance.
Look for a rocker sole. Shoes with a rocker or “speed roll” geometry reduce the amount of flexion at the forefoot during push-off. Hoka’s Meta-Rocker and Altra’s rocker designs are good examples.
Wide toe box. The forefoot needs room to splay during impact. Narrow toe boxes crowd the metatarsal heads. Look for Altra’s FootShape toe box or models available in wide widths.
Adequate stack height. At least 25–30 mm of forefoot cushioning. More is generally better for metatarsalgia, as long as the shoe remains stable.
Removable insole. You need to replace the stock insole with a supportive orthotic insole. Many running shoes have glued-in insoles that are difficult to remove — check before buying.
Cross-Training Options
While recovering from metatarsalgia, these activities maintain fitness without aggravating the forefoot:
Swimming. Zero impact. Excellent for maintaining cardiovascular fitness.
Cycling. Low forefoot load. Ensure your cycling shoes have a stiff sole and do not squeeze the forefoot.
Elliptical trainer. Mimics running motion without impact. Start with low resistance and gradually increase.
Rowing. No forefoot loading. Good for full-body conditioning.
Avoid: basketball, tennis, jumping rope, and HIIT classes until fully recovered.
Quick Note
Many runners worry that taking 2–4 weeks off will cause significant fitness loss. In reality, cardiovascular fitness declines measurably only after 2–3 weeks of complete inactivity, and strength holds longer. Cross-training during recovery preserves most of your fitness while allowing your forefoot to heal.
Conclusion
Metatarsalgia is one of the most common running-related injuries, but it is highly treatable with the right approach. Replace your shoes on schedule, increase mileage gradually, maintain calf flexibility, and use supportive insoles with metatarsal pads. If you develop forefoot pain, catch it early — rest, ice, and insoles can resolve most cases within 2–4 weeks before they become chronic.
Keep running with the right foot support.
Our orthotic insoles with metatarsal domes provide the forefoot relief runners need to stay on the road.
Free returns on all orders · 30-day money-back guarantee
Frequently Asked Questions
Can I run through metatarsalgia pain?
No. Running through metatarsalgia pain prolongs recovery and can lead to more serious injuries such as stress fractures. Stop running at the first sign of forefoot pain, treat it conservatively, and use the walk-run progression to return safely.
Do I need different running shoes for metatarsalgia?
Probably yes. Running shoes with a rocker sole, wide toe box, and adequate cushioning (25–30 mm+ forefoot stack height) are ideal for metatarsalgia. Hoka, Altra, and Brooks offer models with these features. Replace your running shoes if they have more than 300–500 miles on them, as worn cushioning is a common cause of metatarsalgia.
Is forefoot striking bad for metatarsalgia?
Forefoot striking increases load on the metatarsal heads compared to heel striking. If you naturally forefoot strike and have no pain, it is fine. If you develop metatarsalgia, you may need to modify your gait or ensure you have maximal forefoot cushioning.
How long should I wait before running after metatarsalgia?
Wait until you can walk pain-free for several consecutive days, then begin the walk-run progression. Rushing back too soon is the most common cause of recurrence in runners.
Can orthotic insoles help runners with metatarsalgia?
Yes. Insoles with metatarsal domes reduce forefoot pressure by 20–40% and are one of the most effective treatments for running-related metatarsalgia. Replace your running shoes’ stock insoles with supportive orthotic insoles before your next run.