What Is Metatarsalgia? Causes, Symptoms & Treatment Options
What Is Metatarsalgia? Causes, Symptoms & Treatment Options
Metatarsalgia is one of the most common foot conditions — yet most people have never heard of it until they develop the telltale burning ache in the ball of their foot. If you are experiencing forefoot pain, understanding what metatarsalgia is, what causes it, and how to treat it is the first step toward relief.
Key Takeaways
- Metatarsalgia is inflammation and pain in the metatarsal heads — the knobby ends of the long bones behind your toes
- It is not a single disease but a symptom complex with multiple possible causes
- The primary mechanical driver is excessive pressure on the forefoot during walking or standing
- Conservative treatment — supportive insoles, proper footwear, and stretching — resolves the majority of cases
- If left untreated, metatarsalgia can lead to compensatory gait changes that cause secondary pain in the knees, hips, and lower back
Metatarsalgia Definition
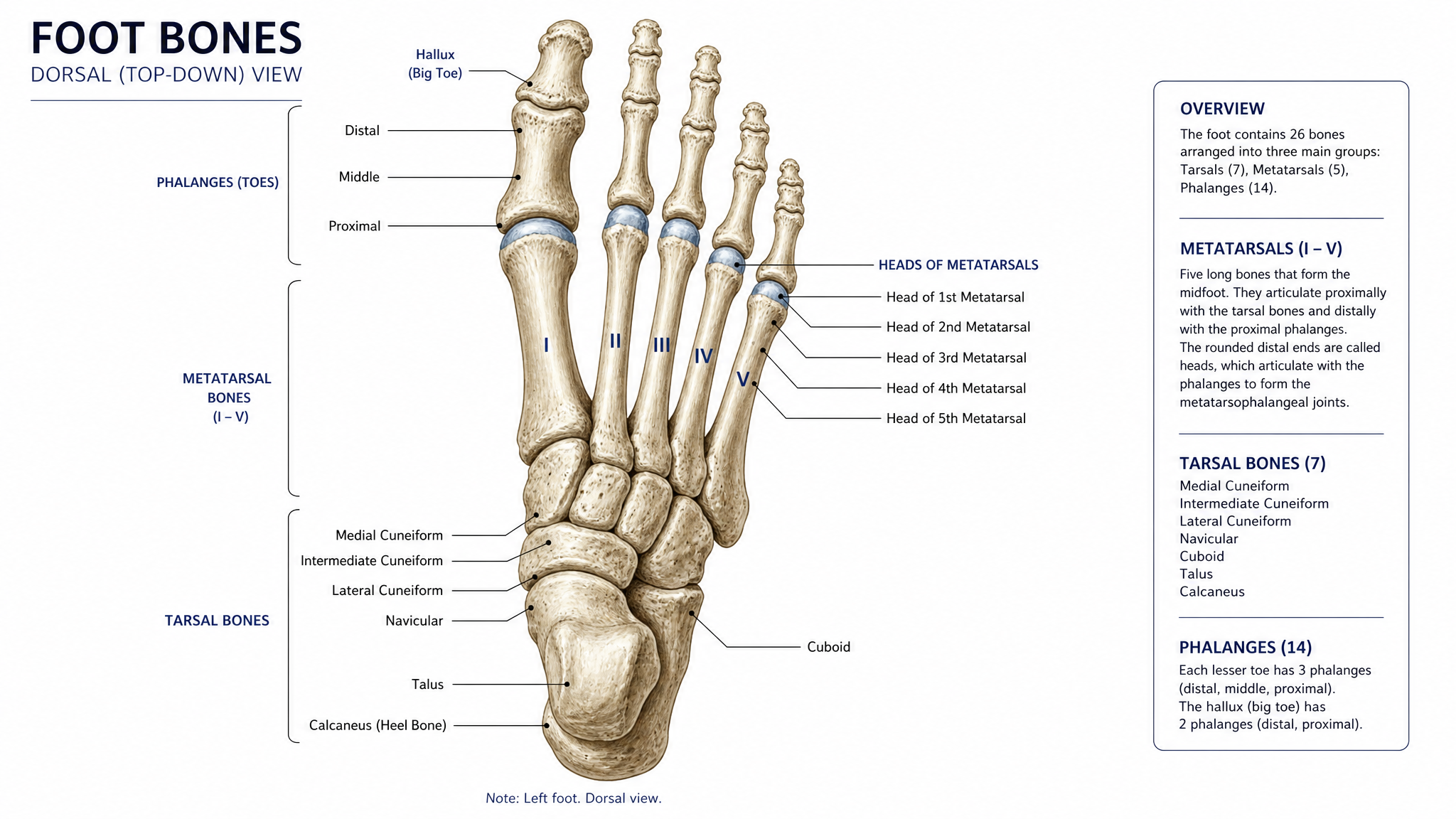
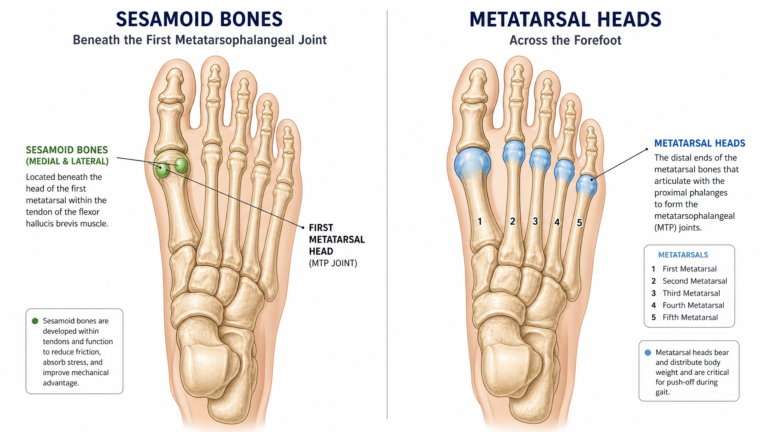
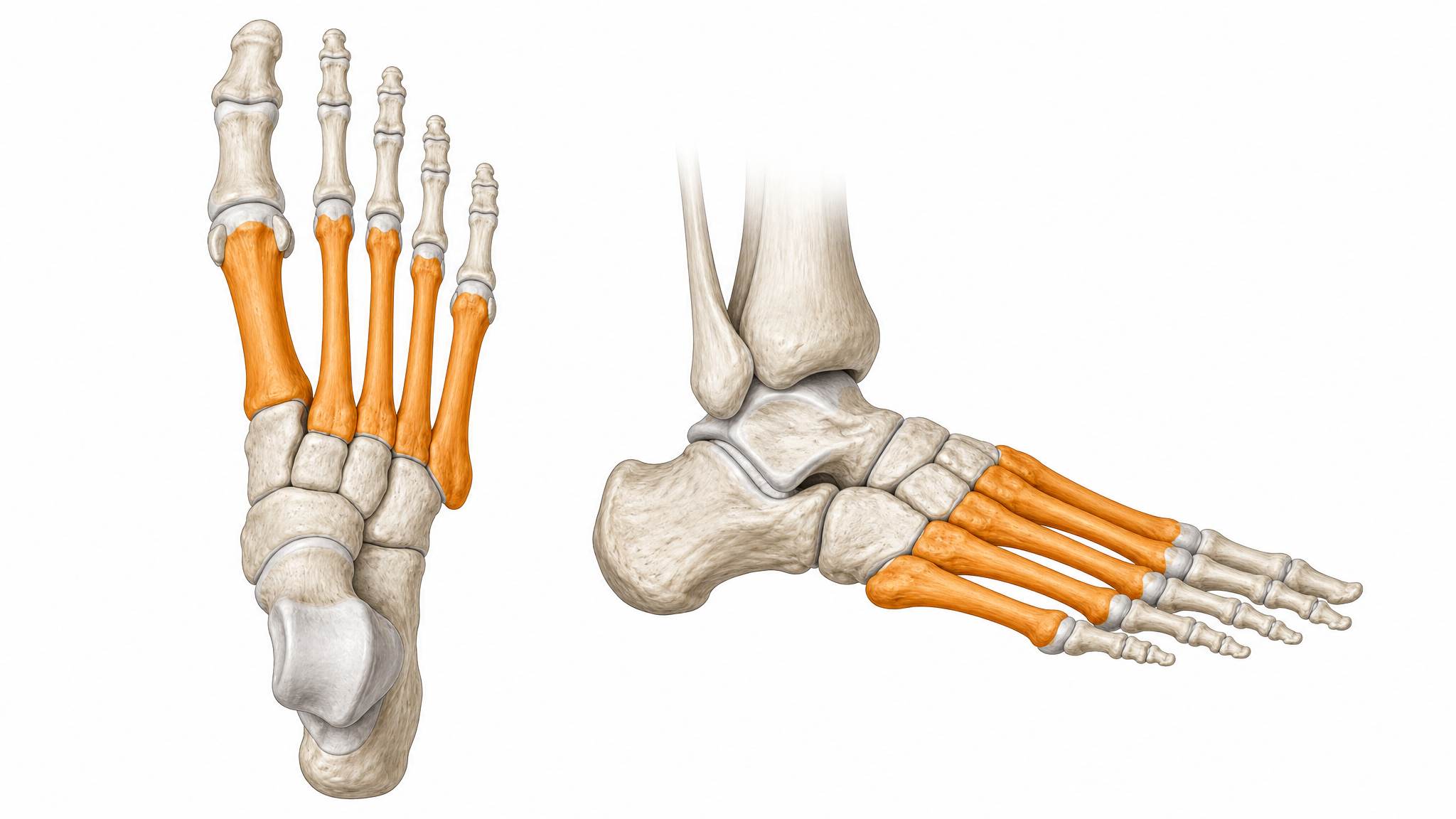
Metatarsalgia comes from “metatarsal” (the five long bones in your foot) and “algia” (pain). It is a general term for pain and inflammation in the ball of the foot — the padded area between your arch and your toes.
The pain involves the metatarsal heads, which are the knuckle-like ends of the metatarsal bones where they connect to your toes. These bones bear a significant portion of your body weight during walking and running. When something causes excessive pressure on them — or reduces the natural cushioning around them — they become inflamed and painful.
Metatarsalgia is not a diagnosis of a specific condition. Rather, it describes a symptom pattern that can result from multiple underlying causes. Think of it like “headache” — the symptom is real, but the cause could be any number of things.
What Causes Metatarsalgia?
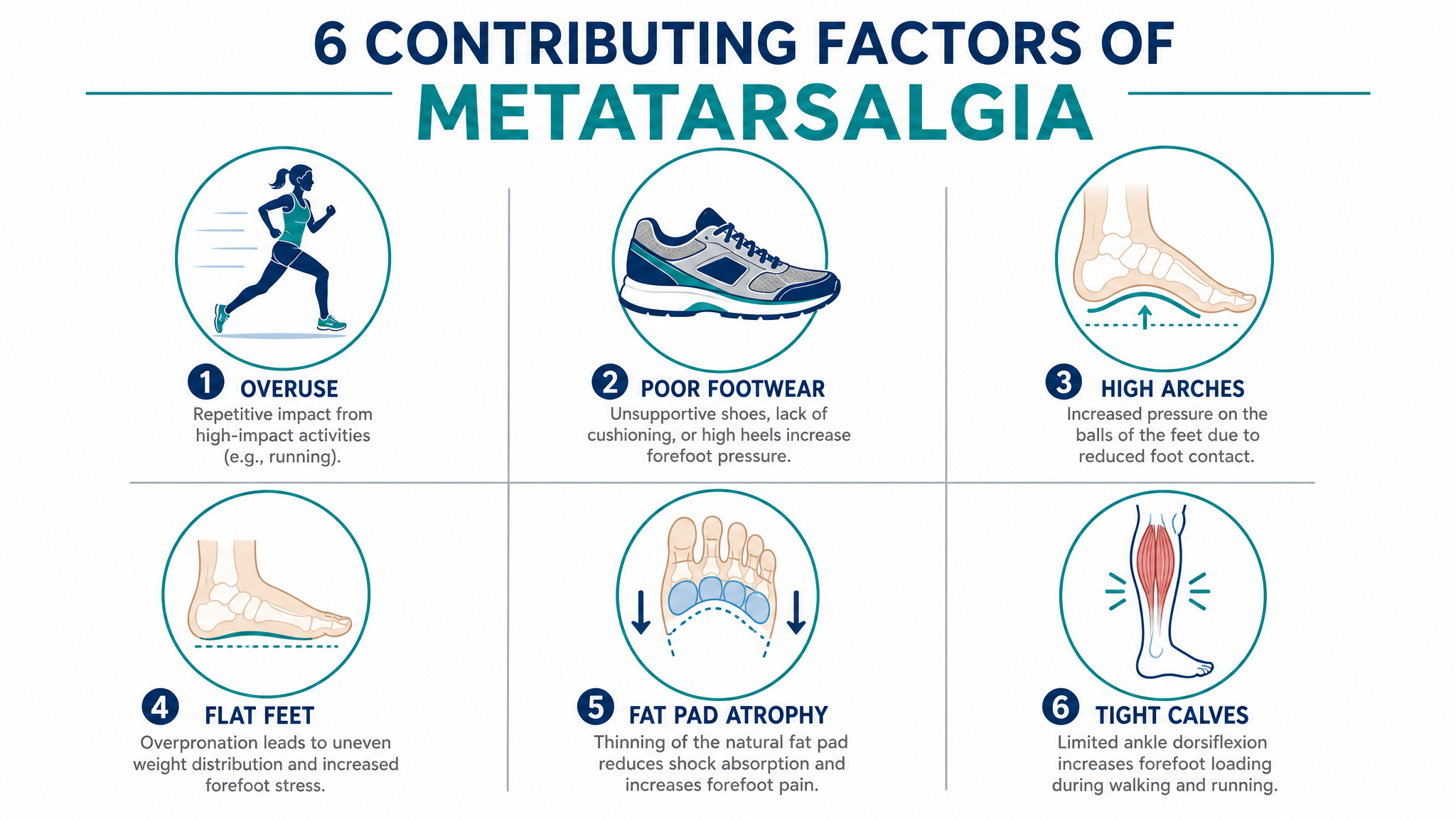
Metatarsalgia develops when the metatarsal heads experience more pressure than they can handle. Several factors can contribute:
Overuse and high-impact activity. Running, jumping, basketball, tennis, and other activities that repeatedly load the forefoot can inflame the metatarsal heads, especially without adequate recovery time or proper footwear.
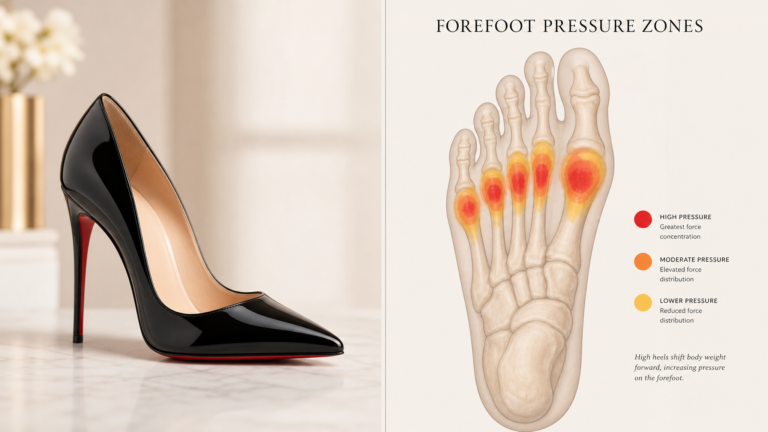
Poor footwear. Shoes with narrow toe boxes crowd the metatarsal heads together. High heels shift body weight forward, multiplying forefoot pressure. Thin-soled shoes provide inadequate shock absorption.
Foot structure. High arches concentrate pressure on the forefoot because the arch does not distribute force effectively. Flat feet cause overpronation that alters weight transfer. Hammertoes and claw toes shift the foot’s natural padding forward.
Fat pad atrophy. The natural fatty pad under the metatarsal heads thins with age — typically starting around age 40. This leaves the bones with less natural cushioning.
Tight calf muscles. When the calf and Achilles tendon are tight, the ankle cannot dorsiflex fully, forcing the foot to compensate by rotating onto the forefoot earlier and staying there longer during walking.
Excess body weight. Higher body weight increases the baseline pressure on the metatarsal heads with every step.
Common Symptoms

Metatarsalgia produces a characteristic set of symptoms:
- Burning or aching pain in the ball of the foot that worsens with standing, walking, or running
- Sensation of “walking on pebbles” or having a stone in your shoe
- Pain that eases with rest and returns with activity
- Tenderness when pressing on the metatarsal heads
- Sharp or shooting pain that may radiate toward the toes in more severe cases
- Numbness or tingling in the toes when nerve involvement is present
The pain typically develops gradually over weeks or months. A sudden onset of sharp forefoot pain — especially after an injury — may indicate a stress fracture rather than metatarsalgia.
Important
If your forefoot pain came on suddenly, followed an injury, or is accompanied by significant swelling or bruising, you may have a stress fracture. See a podiatrist for imaging rather than attempting home treatment.
How Metatarsalgia Is Diagnosed
Diagnosis typically involves a physical examination and, if needed, imaging studies.
Physical exam. Your podiatrist will press on the metatarsal heads to identify tender areas, assess your foot structure (arches, toe alignment), check ankle range of motion (looking for tight calf muscles), and perform specific tests to rule out other conditions (Mulder’s sign for neuroma, vertical stress test for plantar plate injury).
Imaging. Weight-bearing X-rays assess bone alignment and can detect stress fractures. Ultrasound can identify neuromas and soft tissue issues. MRI provides the most detailed view and is used when the diagnosis is unclear or when soft tissue injury is suspected.
Treatment Options

The majority of metatarsalgia cases resolve with conservative treatment. Here are the most effective options, in order of priority.
1. Supportive Insoles with Metatarsal Pads
Insoles are the first-line treatment for metatarsalgia. The key feature is a metatarsal pad (dome) — a raised cushion positioned just behind the metatarsal heads. This lifts and spreads the metatarsal bones, reducing pressure by 20–40%.
The best insoles for ball of foot pain combine a metatarsal dome with firm arch support. This addresses the forefoot pressure directly while also correcting any underlying arch mechanics that may be contributing.
2. Footwear Changes
Switch to shoes with wide toe boxes that allow your toes to spread naturally. Look for rocker sole designs that reduce forefoot flexion during walking. Avoid shoes with heels above 1.5 inches.
3. Stretching and Exercise
Tight calf muscles are a major contributor to metatarsalgia. Daily calf stretches — both straight-leg and bent-knee versions — reduce forefoot pressure by improving ankle range of motion. Strengthening the intrinsic foot muscles through towel curls and marble pickups further supports the forefoot.
4. Activity Modification
During the acute phase, reduce high-impact activities. Switch to swimming, cycling, or elliptical training until the pain subsides. When returning to running or jumping activities, increase intensity gradually.
5. Professional Treatment
If conservative treatment does not provide relief after 6–8 weeks, a podiatrist may recommend:
- Custom orthotics with specific metatarsal accommodations
- Corticosteroid injections for severe inflammation
- Physical therapy for gait retraining and strengthening
- Taping to offload the metatarsal heads
Surgery is rarely needed for metatarsalgia and is typically reserved for cases involving an underlying structural issue that does not respond to other treatments.
How Long Does Metatarsalgia Last?
Recovery time depends on the cause, how long you have had symptoms, and treatment consistency:
- Acute cases (symptoms less than 4 weeks): 2–4 weeks with insoles, activity modification, and stretching
- Subacute cases (symptoms 4–12 weeks): 4–8 weeks, may need insoles plus physical therapy
- Chronic cases (symptoms over 3 months): 8–16 weeks, may require custom orthotics
Consistent daily treatment produces significantly faster results than intermittent treatment.
Can Metatarsalgia Go Away on Its Own?
Mild cases may improve with rest and better footwear, but metatarsalgia typically requires active treatment. The underlying mechanical factors — tight calves, poor footwear, foot structure issues — do not resolve on their own. Without addressing the cause, symptoms usually return when normal activity resumes.
The good news: metatarsalgia is highly treatable. With the right combination of supportive insoles, proper footwear, and targeted stretching, the vast majority of people experience significant relief within 4–8 weeks.
Metatarsalgia Causes Diagram
To visualize how metatarsalgia develops:
- Tight calves → limited ankle motion → early forefoot loading
- Poor footwear → forefoot compression → increased metatarsal pressure
- High arches → poor shock absorption → concentrated forefoot force
- Flat feet → overpronation → altered weight transfer
- Fat pad atrophy → reduced natural cushioning → bone-on-bone sensation
- Overuse → inflammation → pain and swelling
Each factor independently increases forefoot pressure, but they frequently combine. For example, someone with tight calves and flat feet who wears narrow shoes and runs regularly is at much higher risk than someone with only one of these factors.
The most effective treatment identifies and addresses all contributing factors simultaneously.
Quick Note
Metatarsalgia affects an estimated 15–30% of adults at some point. It is particularly common in runners, people over 40, women (due to footwear choices), and those who stand for long hours on hard surfaces. Recognizing it early and starting treatment promptly leads to the best outcomes.
Conclusion
Metatarsalgia is ball of foot pain caused by excessive pressure on the metatarsal heads. It is a common, treatable condition that responds well to conservative treatment — especially supportive insoles with metatarsal pads, proper footwear, and targeted stretching. Most people experience significant improvement within 4–8 weeks of consistent treatment. If your pain persists beyond that, see a podiatrist for a more specific diagnosis.
Start treating your metatarsalgia today.
Our orthotic insoles with built-in metatarsal support provide the first-line treatment for ball of foot pain.
Free returns on all orders · 30-day money-back guarantee
Frequently Asked Questions
Is metatarsalgia a form of arthritis?
No. Metatarsalgia is inflammation of the metatarsal heads (bone ends), not arthritis of the joints. However, inflammatory arthritis conditions like rheumatoid arthritis can cause secondary metatarsalgia due to joint inflammation and toe deformities.
What happens if metatarsalgia is left untreated?
Untreated metatarsalgia typically worsens over time. The pain may increase, and you may develop compensatory gait changes that cause secondary problems in the knees, hips, or lower back. Chronic cases are harder to treat and may require more intensive intervention.
Can metatarsalgia affect both feet?
Yes. Metatarsalgia frequently affects both feet, especially when the cause is systemic (foot structure, body weight, footwear) rather than related to a specific injury on one side.
Is walking good for metatarsalgia?
Walking in supportive shoes with metatarsal insoles is fine and helps maintain mobility. Walking in unsupportive footwear — thin soles, narrow toe boxes, or high heels — will aggravate the condition.
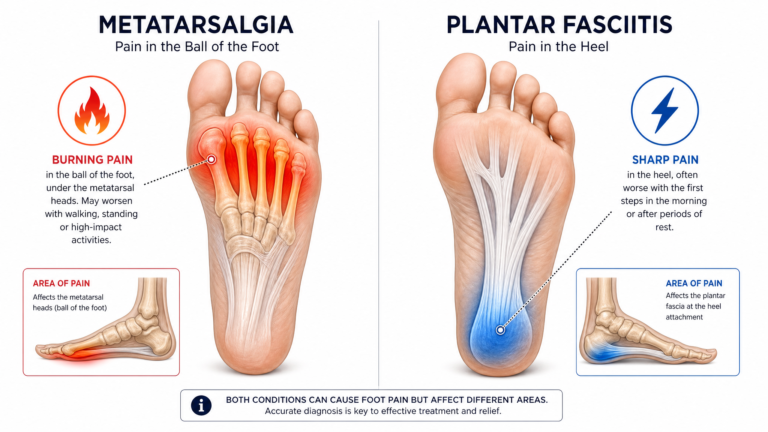
What is the difference between metatarsalgia and Morton’s neuroma?
Metatarsalgia involves inflammation of the metatarsal bones; Morton’s neuroma involves thickening of the nerve between the toes. Metatarsalgia produces broad aching pain; Morton’s neuroma produces sharp, electric, or tingling pain that radiates into the toes. See our metatarsalgia vs Morton’s neuroma guide for more detail.